

Introduction:
Hodgkin lymphoma (HL) is a hematological malignancy, with an inflammatory majority component of reactive cells and a few (1-2%) Reed-Sternberg cells (RSC). A high percentage of patients are cured with conventional strategies but approximately 15-30% relapse or progress. The standard tool to assess disease burden is the Ann Arbor Stage that classically categorizes HL in early (I-II) and advanced stages (III-IV). However, AA staging lacks accuracy in predicting outcome. New ways to asses tumor burden, such as baseline fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT), detect active disease with higher sensitivity in comparison with computed tomography (CT). Additionally, different volumetric parameters, such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG), may be obtained from FDG PET/TC. We aim to improve disease burden testing using FDG PET/TC-related parameters, to better stratify HL patients at the time of diagnosis.
Methods:
We retrospectively selected patients with HL, homogeneously treated with ABVD +/- RT, at Son Espases and Son Llatzer University Hospitals in Palma de Mallorca from the databases of Pharmacy, Pathology and Nuclear Medicine Departments, to avoid selection bias. FDG PET/TC was done at baseline. MTV was measured with a semiautomatic method using a 41% maximum standardized uptake value (SUVmax) threshold and represents the sum of metabolic volumes of tumor tissues with increased FDG uptake. TLG was calculated by multiplying MTV and the mean SUV (SUVmean) of the MTV and was representative of the metabolic activity throughout the entire tumor. We used receiver operating curves (ROC) analysis to obtain the optimal cutoff for progression or death of all experimental FDG PET/TC-related variables. Standard clinical prognostic variables were obtained from medical records (age, gender, stage, bulky and ECOG PS) and main prognostic scores (IPS, EORTC and GHSG) were calculated. Progression-free survival (PFS) was considered the time from diagnosis to disease progression or death of any cause. Univariate survival analysis was done using Kaplan-meier plots and comparison between variables with log-rank test.
Results:
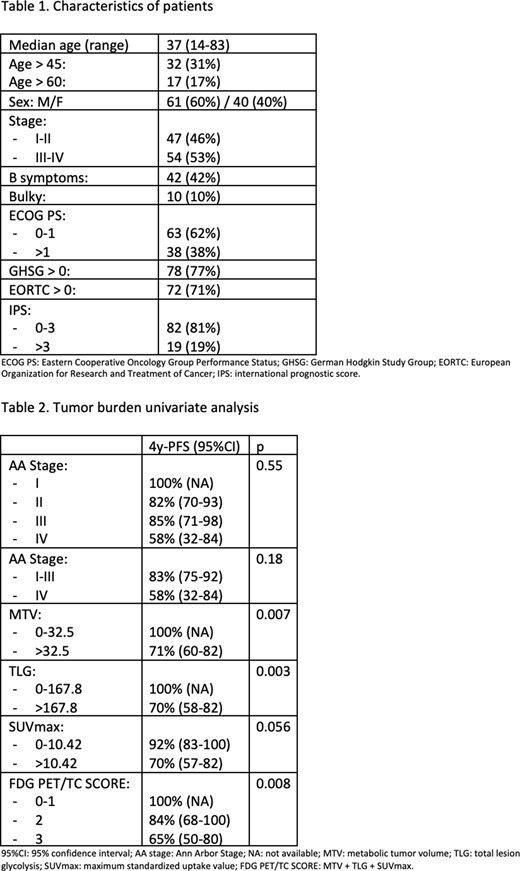
From August-2011 to November-2018, we included 101 patients. Table 1 shows main characteristics of patients. Median age was 37 years (14-83 years), 53% of patients had an advanced stage and 10% had bulky disease. With a median follow-up of 45 months (11-90), median PFS was 78%. The optimal cuttoffs obtained for MTV, TLG and SUVmax were 32.5, 167.8 and 10.4, respectively. In the univariate survival analysis, PFS was significantly influenced by MTV (p=0,007) and TLG (p=0.003), but not AA stage (Table 2). OS was significantly influenced by TLG (p=0.007) and SUVmax (p=0.001). With the three FDG PET/TC-related variables influencing HL survival we designed a FDG PET/TC score as follows: 1 point for high level of MTV, TLG or SUVmax (from 0 to 3). As shown in Table 2, this new FDG PET/TC score had a much better risk assessment that standard AA stage, being able to differentiate three risk groups with 100%, 84% and 65% 4-y PFS and 100%, 84% and 75% OS.
Conclusions:
The combination of functional 3D measurement of tumor burden (MTV, TLG and SUVmax) obtained from the FDG PET/TC at diagnosis, in HL, could be a valuable tool to better stratify the risk patients from tumor burden at the moment of diagnosis, when compared with standard AA staging.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal